

Do you want to sit in the waiting room with your chest pain?
Then vote "Yes" on Trump's BBB

The big, beautiful bill is going to crush Emergency Departments across the country, and here’s why.
As an Emergency Medicine physician at an academic medical center, a large part of what I do in between the heart attacks and car crashes is teach medical students and residents (apprentice physicians who have finished medical school and are in training in their chosen specialty). Most of them will come to the Emergency Department for about a month, working a certain number of shifts to learn some rudimentary Emergency Medicine. I teach them medicine, but no one gets away from a shift with me without hearing me explain EMTALA.

What is EMTALA? It’s what makes Emergency Medicine, Emergency Medicine. EMTALA is the Emergency Medical Treatment and Active Labor Act, and it’s the law. Passed in 1986, the point of EMTALA is that you can’t turn away someone with a life-threatening medical emergency because they are unable to pay. It came about because that’s exactly what hospitals were doing in the early 80s, and there were horror stories of people walking into an ER with a knife sticking out of their head or crowning in labor who were told, “Sorry, but you can’t come in here!” The point of the law is you can’t “dump” patients to different hospitals because someone can’t pay in a true medical emergency, and it does this by requiring ANYONE who checks into an ER to be seen by a medical provider. That’s someone with an independent medical license, not a nurse, not a medical student, etc.
And what we’re required to do is evaluate the patient for a life threat or active labor and if we identify that, we’re REQUIRED to try to stabilize it. It also governs transfers in between hospitals, as you can imagine, one could evaluate someone and immediately transfer them if they didn’t have the ability to pay (that was happening a lot too in the 80s).
And that, at the root, is why Emergency Departments exist. It’s not for your sprained ankle, or your ingrown toenail, or your migraine. Now, OF COURSE, we see all those people too, because most of what we do in the ED is provide “unscheduled care” and not “emergent care.” And EMTALA only applies to the ED (you can croak on the doorsteps of your PCP and they aren’t legally required to do anything).
This has all sorts of ramifications for why the Emergency Department practices medicine the way we do. Patients see the repercussions for this in long wait times. Why did you sit in the ED for 6 hours? Well, if someone was potentially sicker than you, they go to the front of the line, and you wait. EMTALA also means the Emergency Department fosters, prioritizes, and expects a culture of clinical sensitivity and sacrifices clinical specificity. This means we need to prove to ourselves (and the patient) that your headache isn’t a brain bleed, that your chest pain isn’t a heart attack, that your car accident didn’t break your neck. We’re terrified of missing something, the big sin in Emergency Medicine is missing a life threatening etiology, while EVERYWHERE else in medicine the big sin is DOING something that results in harm (incidentally these competing motivations are why every other field of medicine buts heads with us when we call them at 3 am).
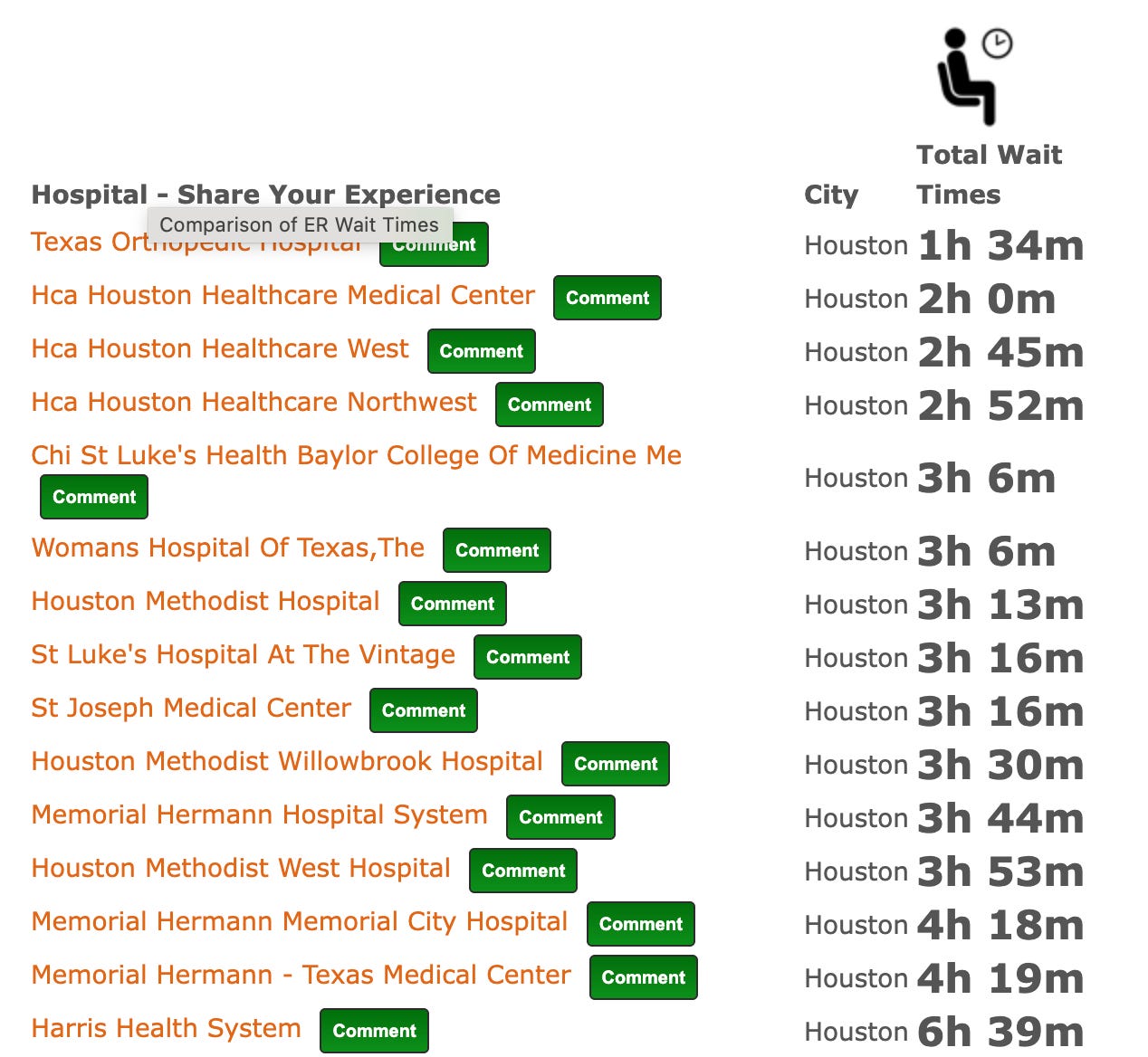
Which brings me, finally, to the Big, Beautiful Bill. Cutting MEDICAID for 17 million people is going to result, not in those people avoiding medical care, but it is going to make them go to the one and only place in town that is both required by law to stay open 24/7 but also required by law to see them, no matter what. Emergency Departments are underwater as is, with average wait times to be seen running, conservatively, in the 3+ hour range across large hospitals. Moreover, the BBB is limiting loan repayment programs such as the Public Student Loan Forgiveness and limiting student loans for 4 years of residency. What this means, if you aspire to be any type of surgeon, you’re going to get hammered with student loan repayment while you’re still getting paid as a resident (a neurosurgical residency is 7 years for example).
During COVID, when the goal was to “flatten the curve,” and only go to the hospital if you were actually dying, I had a patient. He was a young guy, mid-30s. He had an infection. It started as a red spot on his leg, he told me. He was sick, he hadn’t come in to see his doctor because he didn’t want to go “where all the COVID people are.” He was diaphoretic, breathing fast, and feeling woozy. When I palpated the red spot, which now had thin blisters and weeping fluid, my finger sunk into his leg.

He had necrotizing fasciitis. I immediately called out surgeons, who had him in the operating room within an hour; the infection had tracked from his shin all the way up under his skin into his armpit. His torso had rotted. He died on the table when his blood pressure tanked.

If he had gone to his primary care physician when it was just a simple red spot, he’d be alive today with just an empty bottle of doxycycline in his medicine cabinet that someday he’d throw out and try to remember what it was from. Instead, he died painfully and horribly. That’s what happens when people can’t access a primary care doctor.
The BBB is going to fuck Emergency Departments, and that means its only a matter of time before it fucks you.
ERs are already over taxed because primary care in America inadequate. When you destroy Medicaid untreated illnesses will be epidemic and ERs will be overwhelmed. This is evil.
God help us. I pray everyday for our country. For healing of the greed and hatred.